SPECIAL HOSPITAL SVETI VID has introduced new era of glaucoma surgery, changing old and non-efficient surgical procedures.
This new era has started with new method using miniature intraocular implants (MIGS), after which the patient achieves new comfort in life, without using eye drops, which makes a big difference comparing to old methods when patients suffered from allergic reactions on eye drops.
In special hospital SVETI VID this surgery is performed by experienced European surgeons, who have special license which is necessary for performing this type of surgery.
Glaucoma in the widest sense implies a group of diseases resulting in damage of the optic nerve with loss of visual function and ultimate blindness, if not treated. These diseases are MULTIFACTORIAL with a wide range of risk factors where the elevated intraocular pressure is only one of them.
Symptoms
Most frequently it is chronic and begins insidiously, without noticeable symptoms in the beginning, painless, yet leaving alarming number of blind people of various age.
When confronted with diagnosis, patient first reaction is unbelief. The sight initially has not been compromised. Elevated intraocular pressure, as most frequent manifesting sign of disease, except in twice increased then normal values, does not bear pain.
In acute condition, accompanied with high intraocular pressure, the eye is “hard on touch”, painful, with severe pain spreading toward the entire half of the head, followed by nausea and vomiting.
Glaucoma strikes first at peripheral vision, therefore the peripheral visual field defects are detected, whereas central vision remains preserved. That is why the first symptoms are “silent”. When the pain occurs and visual field defect becomes apparent, the significant irreversible damage to the optic nerve has already occurred.
At this moment the target of the therapy is to halt the disease at present stage, and keep the intraocular pressure under control. It is essential to demystify the problem and help the patient understand the disease, because only then he will understand the necessity for timely treatment. Glaucoma is lifelong, but prompt and proper care will make possible normal life with a disease that is kept under control (such as high blood pressure).
When glaucoma develops
The contemporary ophthalmology means detection, as early as possible, of the initial symptoms and signs of possible glaucoma, and thereafter with wide range of subtle diagnostic procedures, to confirm or exclude the disease, at the moment.
At the earliest stage there are changes on the level of the retinal ganglion cells!
There are many predisposition factors and risk factors for development of some of a few types of glaucoma.
Basically, there is a defect in vascular supply because of perfusion disorders, upon which the neural cell is highly sensitive. Its sensitivity is greater in cases of elevated IOP or oscillations in the IOP. Perfusion disorders exist with circulation problems, such as carotid arteries stenosis, decreased blood pressure and high myopia respectively.
These risk factors can intensify the damage, yet all this means not that all patients with circulation problems necessarily have glaucoma. Genetics will dictate the behavior and sensitivity of these fine structures in the frame of all present risk factors.
Risk factors
Increased IOP is considered the main risk factor, but not the only one.
Old concept that increased values of intraocular pressure with optic nerve damage and typical glaucomatous “defect” in visual field constitute glaucoma is somewhat deficient and has changed today. Increased IOP will accelerate the development of glaucomatous damage, yet glaucoma IS NOT the same as increased intraocular pressure, by itself. Some records show fine changes in the optic nerve structure at the back of the eye (papilla) in conditions of “relative” normal or even lower IOP.
That is so called normal or low- tension glaucoma. Values of IOP from 9-21mm Hg are taken for ‘’normal’’ by concensus, which means that 95% of people without glaucoma have the values with that range of IOP. The rest without glaucoma can have higher or lower values than above mentioned. Anyway, comprehensive diagnostics are necessarily to exclude glaucoma.
Around 25% of patients with clear glaucomatous defects has pressure within “normal”. That means that the absolute values of IOP cannot be interpreted without necessary data, which means: the grade of damage, positive hereditary anamnesis, the presence of other risk factors, oscillation of IOP during the day etc.
The asymmetry of ocular pressure between eyes, and higher daily fluctuations of pressure are alarming sign, as well as existing asymmetry in PNO appearance even within “normal” values of IOP.
Heredity
Verified damage of the optic disk, or visual field defect, as well as positive family history for glaucoma is an alarm to re-examine whether the measured IOP is the optimal for that person, itself, or has to be lowered.
Therapeutic action is taken when even subtle changes are detected.
Glaucoma types
Elevated eye pressure (“hard eye”) occurs because of disbalance in production and drainage of aqueous humor. Greater production in relation to drainage, respectively harder drainage because of increased resistance in “canals” through which aqueous flows, at normal eye anatomy and angle chamber structure is characteristic of so called open angle glaucoma.
Difficult drainage occurs in conditions of altered chamber angle (narrow or closed angle glaucoma) which can be congenital, or the anatomy is changing with age. Farsightedness with shallow eye chamber is predisposition for glaucoma as well. Secondary glaucoma occurs in ocular inflammations (uveitis) or traumas, because of inflammatory debris in angle chamber. It can be expected as a complication of „maturing“ of cataract, when swollen lens narrows the anterior chamber and angle, or obstructs pupilary region and cuts off the flow of aqueous humor from posterior into anterior chamber.
Should it disintegrate, this cataract can lead to clogging of the chamber angle or secondary inflammatory reaction – uveitis. These all are dangers of obsolete concept about „waiting to mature“ abandoned in ophthalmology in the seventies of the past century. Prevention measurement is an early cataract surgery- phacoemulsification (ultrasound surgery).
Once it was hard to imagine, yet today the changes can be seen with new imaging technology. Necessary diverse testing will give substantial picture and determine gravity of the condition.
OCT – detects EARLIEST, objective, quantitative, degree of primary damages on the level of the ganglion cell, in pre-clinical stage. Therefore, when patient has no symptoms and when it can not be seen with standard visual field testing.
Also, the appearance and thickness of nerve fibers, and degree of excavation (deepening of the cup because of nerve atrophy) in advanced stages.
It is of great importance for following the effects of therapy, and stage and prognosis of the disease.
DIGITAL FUNDUS DIAGNOSTICS provides objective recording of the appearance of the optic nerve head.
CVF – computerized visual field – representation of the degree of functional loss with characteristic „defect“ in visual field.
DAILY CURVE of the intraocular pressure shows fluctuations or stability of the values.
PACHIMETRY –thickness of cornea, necessary for accurate interpretation of the values of intraocular pressure.
The goal of the therapy is protection of the nerve and regulation of the ocular pressure. It starts with ocular drops, and in cases of pending acute attack in cases of angular glaucoma the laser is applied. If maximal therapy does not regulate the disease, the surgery is mandatory.
It is important to react with great speed before the optic nerve is completely destroyed. Surgery on the blind eye is unreasonable.
A physician not familiar with this problem should timely recommend a patient to the right place. Uncritical interpretation of the ocular pressure values not in consistence with degree of damage has disastrous outcome.
By “maximal therapy” we mean all the available possibilities for disease control with medication, considering the age of the patient.
Among younger (30 – 40 years of age) with confirmed worsening of the disease even with two medications, it is recommended to consider surgery. These are people expected to battle the disease for many years, and long-term application of these medications is not completely harmless. Although effective, these medications have side effects, even contraindications.
With long-term therapy “biology” of the tissue undergoes changes thereby diminishing the effect of late performed surgery.
Basic diagnostics, adjusting the IOP values according to the appearance of the optic nerve head, timely start with medication, red-flagging any new atypical change is immeasurable benefit in wise treating of the disease, if seriously undertaken.
These concepts and modern approach to glaucoma treatment, we introduced and instituted center for treatment of this disease with European leading experts in this field – Prof. dr Šarka Pitrova i Prof. dr Pavel Rozsival.
Employing modern possibilities of treatment and surgical procedures this disease is successfully controlled.
Surgical procedure has a target to provide the balance between production and drainage of aqueous humor. The choice of timing and appropriate method or combination of methods depends on type of glaucoma and IOP level aimed to achieve and planned value is determined according to the disease behavior, length of treatment and degree of damage.
Considering the intricacy of the problem this decision should be given to only exceptional experts who know all the subtleties of the problem and govern these techniques. The procedure is decided for each case individually.
Non-critical application, “must be” of always the same, aggressive, not customized surgical technique, certainly adds to increase of blind population here..
A wise choice of adequate surgical method or combination of methods according to each patient individually is prerequisite and most delicate moment in battle glaucoma.
For years Special Hospital SVETI VID, like leading centers for glaucoma in EUROPE is treating this problem according to the modern approaches. Along with outstanding names of European ophthalmology, here are established new sophisticated surgical approaches as modified trabeculectomy procedures, in cases of great damage and decompensated glaucoma, filtration as well as minimally invasive glaucoma surgeries (MIGS), with application of modern mini implants adapted to the stage of the disease.( Ahmed, Ex-press implant, Xen, I-stent,…)
This is the way to overcome risks of obsolete, aggressive, non-customized surgical techniques.
CONGENITAL GLAUCOMA is a serious disease lifelong and leading to blindness if timely action is not taken. It can be detected immediately upon birth or later. Often the parents will notice big-protruding eye-or big cornea, which is under extremely high ocular pressure thinning and clouding.
Ocular cover-membrane in child’s eye is quite elastic, so by increasing dimensions, the eye fairly compensates increased intraocular pressure and saves the optic nerve. Glaucoma is sometimes accompanied with congenital cataract and other anomalies of the anterior segment of the eye.
The surgical procedure is necessary along with therapy by eye drops. Frequent controls are mandatory.
THE LATEST IN GLAUCOMA SURGERY
This type of surgery is performed by experienced European Professors-surgeons, who have over 30 years of surgical experience, which is the best guarantee to patients for the successful surgical outcome.
SPECIAL HOSPITAL SVETI VID introduced glaucoma surgery into new epoch, changing old, deficient surgical procedures. Years ago, that was non-penetrating deep sclerotomy by application of SK gel, and now the employment of modern gel implants, by surgical technique taking place through miniature incision, that heals instantly.
Miniinvasive glaucoma surgery (MIGS) is not advised in terminal, far advanced stages resulting in great nerve damage and significant visual field loss. Optimal effect of surgery is expected in incipient and moderately advanced stages, when usage of one eye medication cannot prevail the disease, so called “unyielding glaucoma”, “resistant” to standard therapy even after the prior surgery that did not bring results.
The disease is to be closely followed, and for that purpose there are modern imaging methods, before all OCT.
Optical tomography is an objective indicator of degree of damage and enables comparative view with prior stages, therefore objectively shows whether the disease is advancing. In such case it is necessary to plan adequate surgical procedure, before serious and definite damages and loss of sight occurs.
MINIATURE XEN-GEL IMPLANT IN MINIMALLY INVASIVE GLAUCOMA SURGERY
Long ago originated the idea of using gel implants that would modify traditional surgical approaches and enable the treatment of glaucoma even in incipient and early phases.


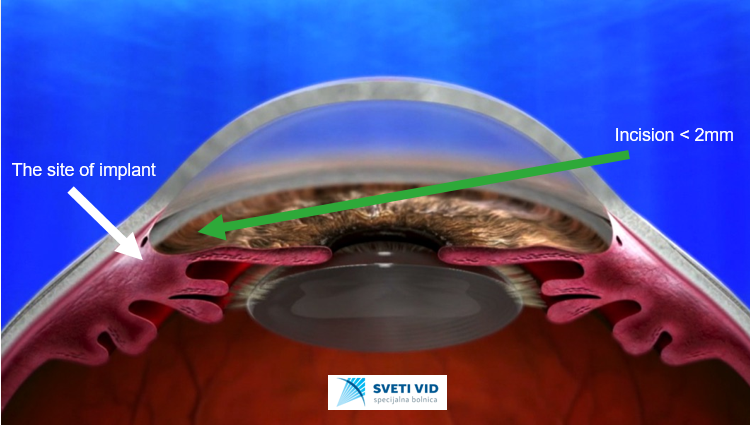
- The aqueous flow from anterior chamber into subconjunctival space
Via 2mm size opening in cornea, like mini-invasive cataract surgery, minuscule injector is placed, containing gel-imlant, 6mm long, 45 microns wide, flexible. It is placed by “micro needle” into subconjunctival space where it remains. This technique “aids” the outflow of the aqueous in space out the eye to be realeased through regular venous way.
The advantage of this method in comparison with earlier methods is that there is no implantation from the “outside”, but inside the eye– ab interno.
Often in combined cataract and glaucoma cases, in planning cataract surgery often is recommended combined procedure, during which Xen implant will be placed therefore stabilizing the eye pressure, and through the same incision will be intraocular implant implanted. The incision is minute, self-enclosing. There is no staying in the hospital.
MICRO-SHUNT GLAUCOMA SURGERY (MIGS) WITH PRESERFLO IMPLANT
Indications are as for any micro-shunt surgery. The approach is ab-externo. The aim of the surgery is to make aqueous outflow from anterior chamber through mini-shunt (70 mcr diameter) into the subconjunctival space to be resorbed.
Therefore, the risk of fibrosis is much less than in classical filtration surgeries (trabeculectomy-TE). Continuous controlled and undisturbed outflow of aquesous humour is achieved.
MIGS with PRESERFLO implant provides comfortable and subtle surgical approach, better intraoperative control of aqueous humour flow, less outflow and less intra- and post-operative risk.
The advantages:
-less invasive that trabeculectomy-TE
-no scleral flap, sclerotomy, iridotomy
-no sutures
-place of the implant in any quadrant is possible

UNFAMILIAR WORDS:
IOP –intraocular, eye pressure
Papilla of the optic nerve, PNO, optic disc – the beginning, the head of the optic nerve
Perfusion – blood supply to the tissue